
Your knee is a hinge joint where the thigh bone (femur), shin bone (tibia) and kneecap (patella) meet. The ends of these bones are covered by articular cartilage, a smooth, slippery layer that lets the joint glide almost without friction and acts as a shock absorber. In osteoarthritis, this cartilage gradually thins, softens and frays. As it wears away, the bones underneath thicken, small bony spurs (osteophytes) form at the edges, and the joint lining can become inflamed and produce extra fluid.
Osteoarthritis is the most common form of arthritis and the knee is one of the joints most often affected. It is often described as "wear and tear", but that is only part of the picture: it is an active process involving the whole joint, and the amount of damage seen on an X-ray does not always match how much pain a person feels. Some people with marked changes on X-ray have modest symptoms, while others with milder changes have significant pain. This is why treatment is guided by how the knee affects your daily life, not by the X-ray alone.

Knee osteoarthritis usually develops slowly over months to years. Common symptoms include:
Symptoms often affect both knees, though one is usually worse. Many people in Delhi first notice it when floor-sitting, using Indian-style toilets, or managing stairs becomes painful.
Osteoarthritis develops when the cartilage's ability to repair itself cannot keep pace with the stresses placed on the joint. Several factors raise the risk:
Often more than one factor is at work at the same time.
See a doctor if knee pain or stiffness is limiting your daily activities, lasts more than a few weeks, or keeps returning. Book an assessment sooner, or seek prompt medical care, if you have any of these red flags:
If a red flag is present, do not wait for a routine appointment.
At VinayakM, diagnosis of knee osteoarthritis is mainly clinical, supported by imaging where it adds value:
The aim of assessment is not just to label the condition but to understand its stage and impact, so the treatment plan fits your knee and your life.
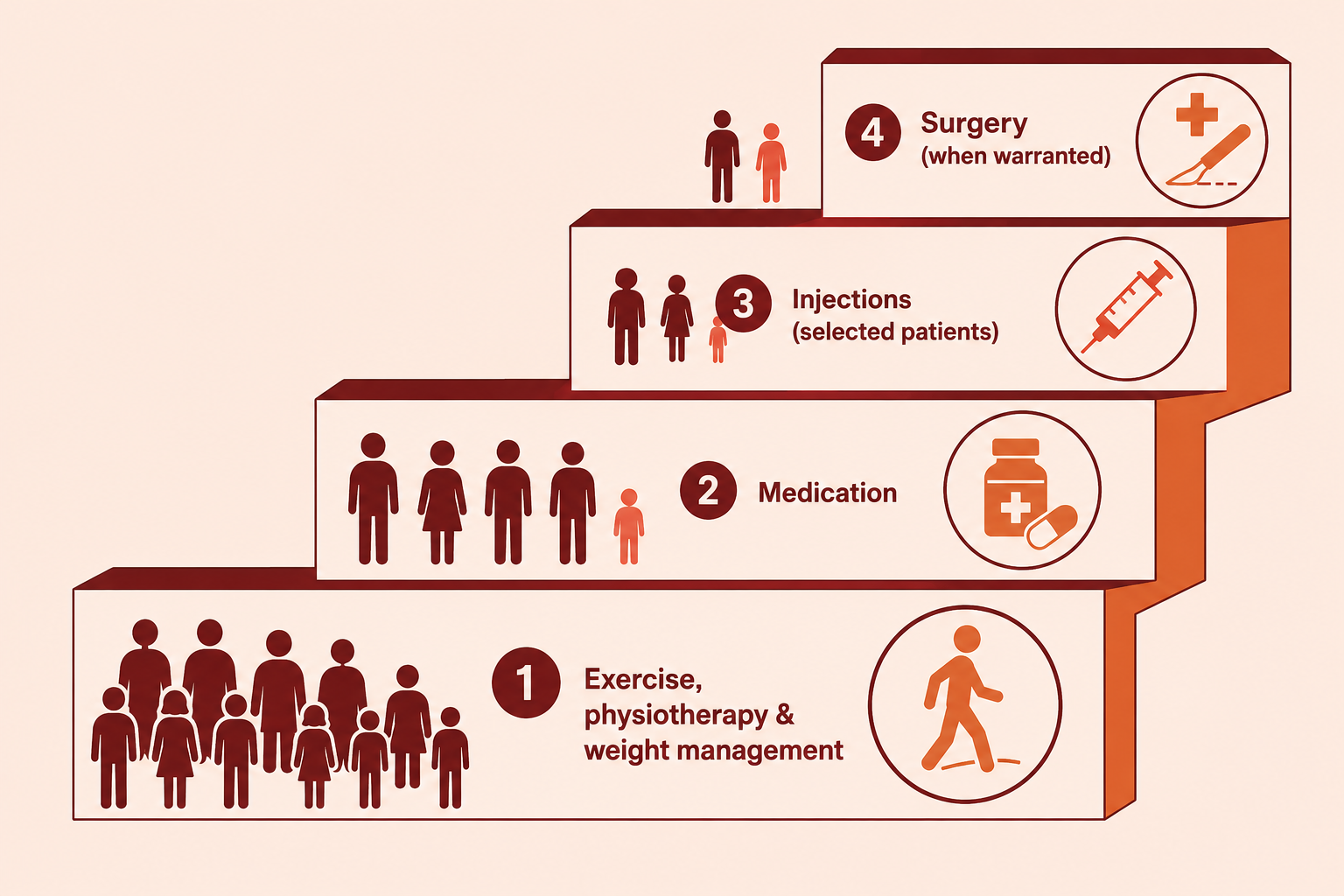
Treatment for knee osteoarthritis follows a stepped approach — start with the safest, least invasive measures, and move up only if symptoms are not adequately controlled. There is no treatment that regrows worn cartilage; the goal is to reduce pain, keep the knee moving and maintain your quality of life.
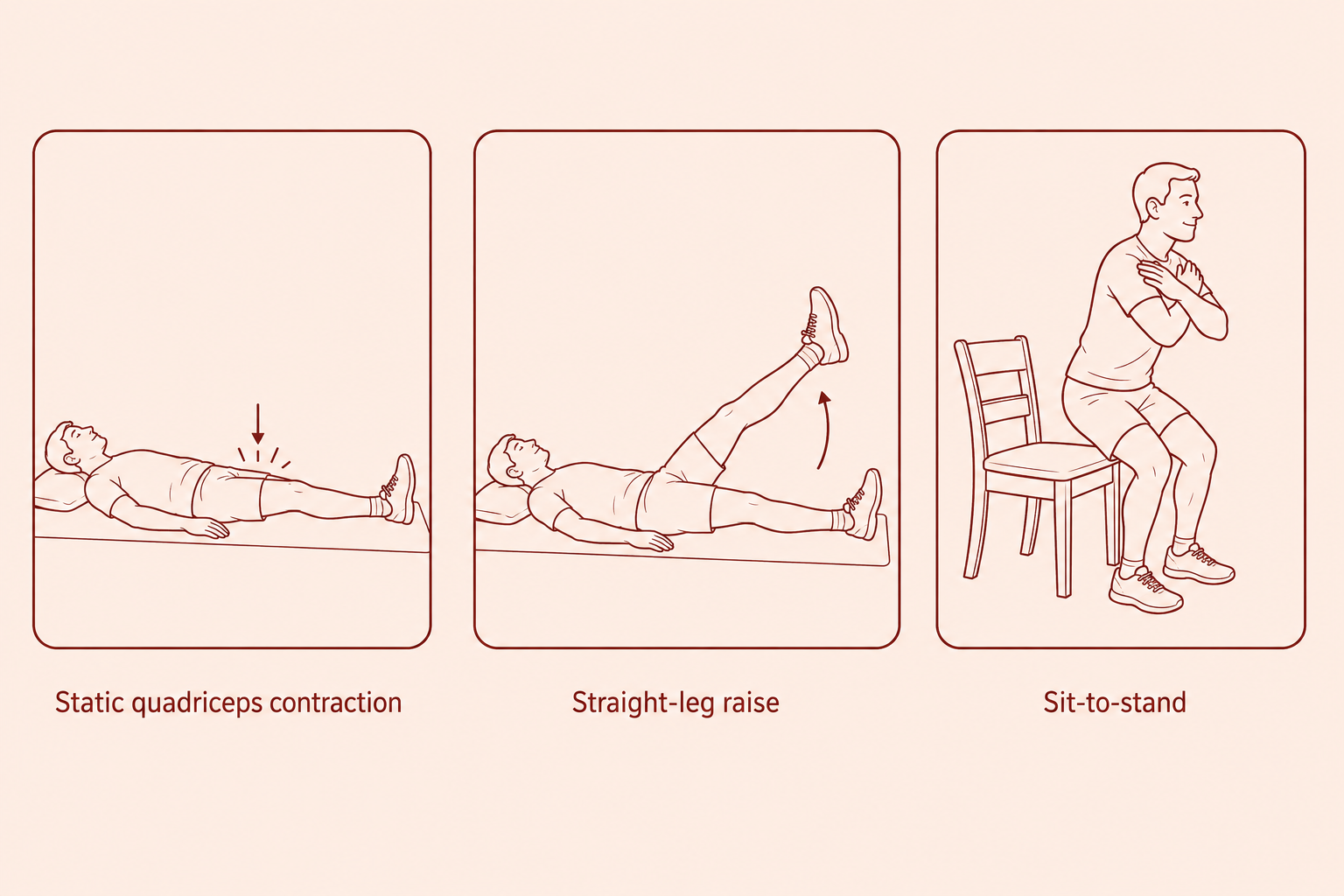
1. Core measures (recommended for everyone):
2. Medication:
3. Interventional (injection) options — considered when core measures and medication are not enough:
4. Surgery — considered when pain and loss of function are significant and have not responded to the measures above:
The right combination differs from person to person, and the plan is reviewed over time as your knee changes.
At VinayakM in Greater Kailash-1, our orthopaedic care for knee osteoarthritis is led by Dr Udit Vinayak, orthopaedic surgeon, and follows this stepped, evidence-based approach rather than jumping to procedures. In practice that means:
We will not promise a cure or a specific outcome. Our aim is to control your symptoms with the least invasive approach that works for you, and to review the plan as things change.
You cannot change your age, sex or family history, but several habits genuinely help protect your knees and ease existing osteoarthritis:
Start new exercises gently and stop anything that causes sharp or lasting pain. If you are unsure what is safe for your knee, ask for a tailored programme rather than guessing.
No. Osteoarthritis cannot be cured and worn cartilage does not grow back. However, the symptoms can usually be controlled well for years with exercise, weight management, physiotherapy and, when needed, medication or injections. The aim of treatment is to reduce pain and keep you active, not to reverse the changes in the joint.
For most people, walking and other low-impact activity are helpful, not harmful. Movement nourishes the cartilage and keeps the supporting muscles strong, and inactivity tends to make stiffness and weakness worse. Build up gradually, wear supportive footwear, and if a particular amount of walking consistently flares your knee, discuss pacing and a tailored programme with your doctor or physiotherapist.
Usually not. Knee osteoarthritis is diagnosed mainly from your symptoms and examination, supported by a standing X-ray. An MRI is only needed if we suspect another problem, such as a meniscus or ligament tear, that would change the treatment plan.
No. Many people manage knee osteoarthritis for years without surgery. Knee replacement is considered only when pain and loss of function are significant and have not responded to exercise, weight management, physiotherapy and other measures. It is a shared decision based on how the knee affects your life, not on the X-ray alone.
They help some people, but the evidence is mixed and they are not suitable for everyone. They are considered in selected patients when core measures are not enough. We discuss the realistic expectations, costs and alternatives before recommending any injection, rather than offering it as a routine fix.
Yes. Being overweight is one of the strongest and most changeable risk factors for knee osteoarthritis, because extra weight increases the load across the knee with every step and fatty tissue also promotes inflammation. For people who are overweight, losing weight can meaningfully reduce knee pain and slow the strain on the joint.
Osteoarthritis is a gradual wear-and-repair problem of the cartilage, usually related to age, load and previous injury, and it typically affects the knees and hands. Rheumatoid arthritis is an autoimmune condition in which the immune system attacks the joint lining, often affecting many joints on both sides with prolonged morning stiffness. They are treated differently, so an accurate diagnosis matters.
