
Back pain is one of the most common reasons people see a doctor, and one of the most misunderstood. The reassuring truth is that the great majority of back pain is 'mechanical' and not dangerous — it comes from the muscles, ligaments, discs and small joints of the spine, and it settles over days to weeks. Modern guidance has moved firmly away from bed rest and early scans towards staying active and confident, because that is what actually speeds recovery.
That said, a small proportion of back pain signals something that needs prompt attention. The practical skill — and the main job of assessment — is to separate ordinary mechanical back pain, which needs reassurance and activity, from the few cases that need urgent care or specific treatment. This page helps you understand both.
Ordinary mechanical back pain typically:
Related patterns include:
The features that matter most, though, are the warning signs in the next section — they change the urgency completely.
Common causes of back pain include:
Stress, poor sleep and low mood also genuinely influence how back pain is experienced and how quickly it settles.
Seek urgent/emergency care if back pain comes with any of these red flags:
Without red flags, see a doctor routinely if pain is severe, is not improving after a few weeks, or keeps recurring and limiting your life.
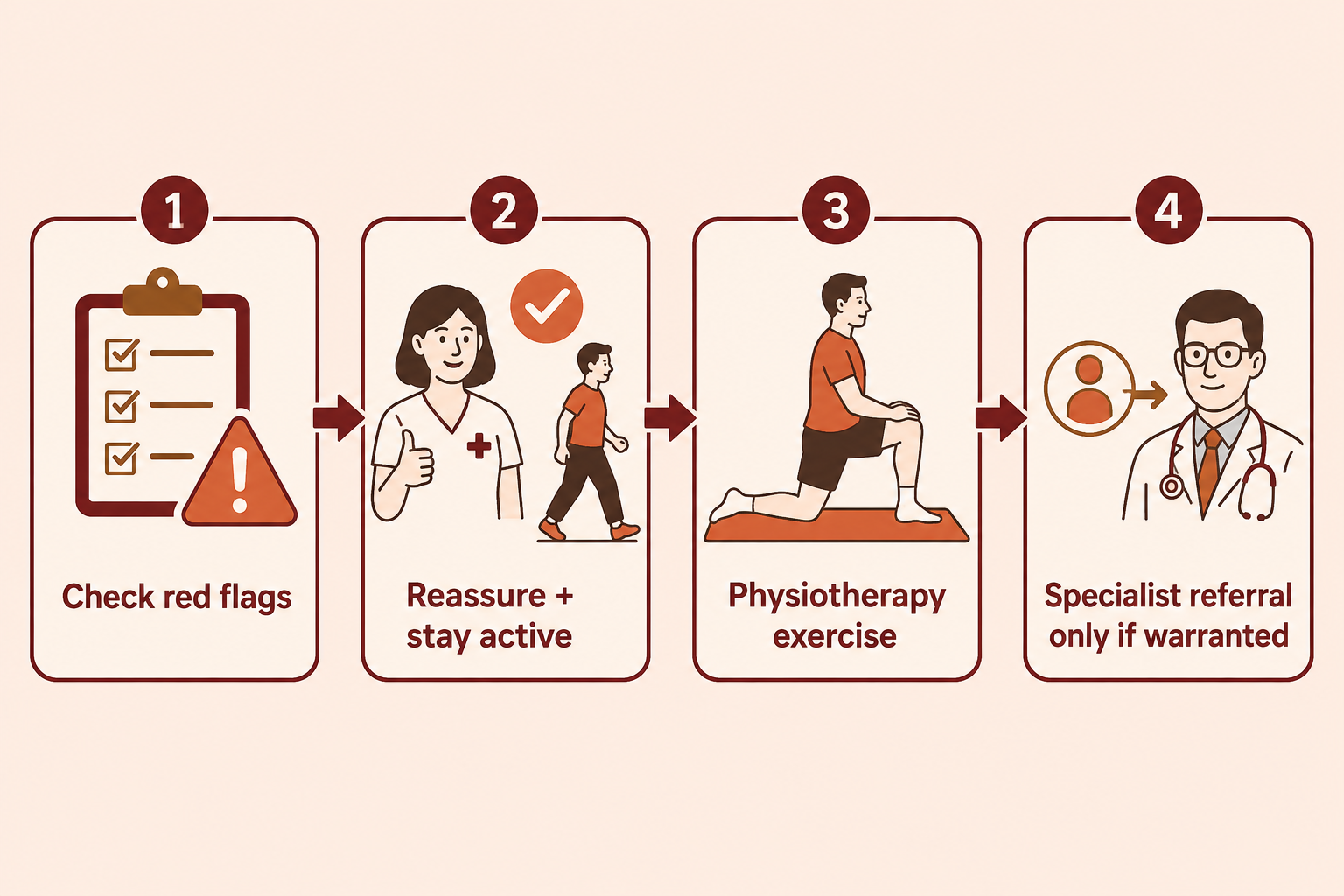
At VinayakM, back pain assessment is guided by ruling out the serious and reassuring the common:
The aim is a confident, safe diagnosis — usually 'mechanical back pain' — and a clear plan, not a scan for its own sake.
For most (mechanical, non-red-flag) back pain, treatment is active and reassuring:
1. Stay active.
2. Simple pain relief.
3. Exercise and physiotherapy.
4. Address the whole picture.
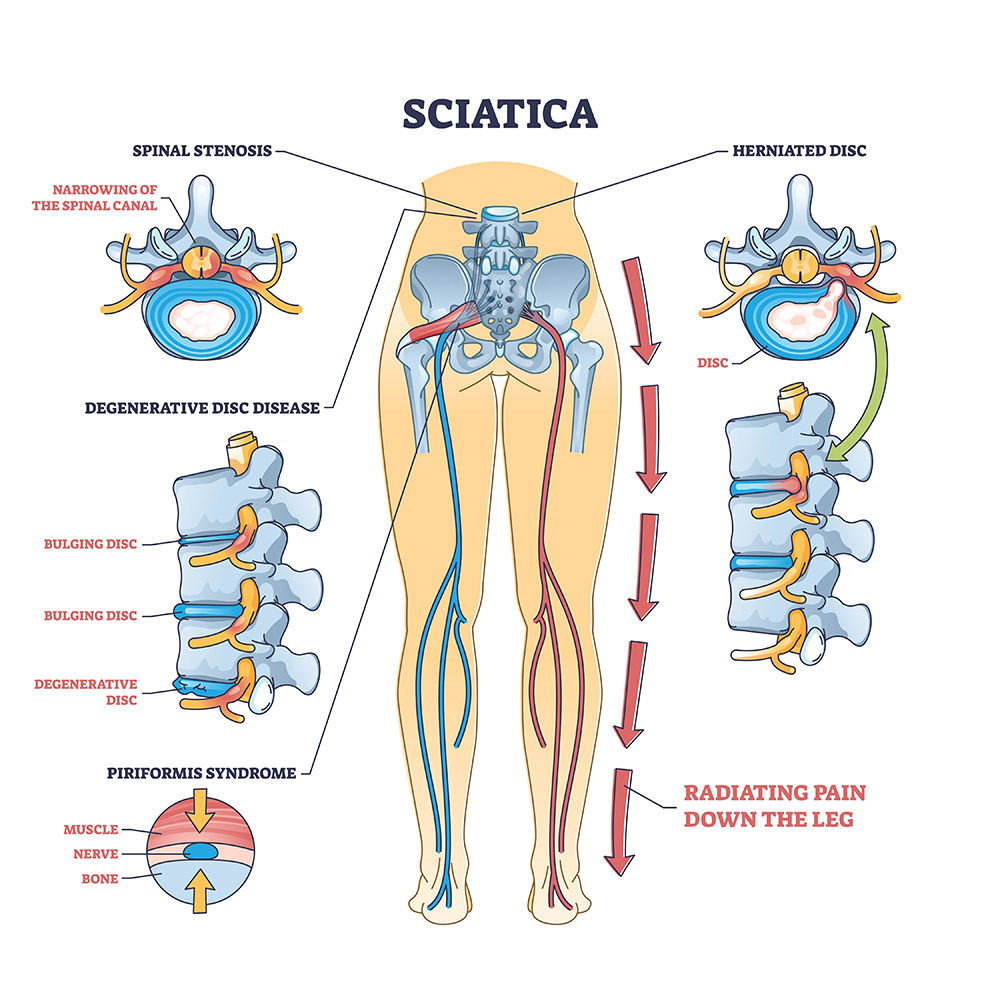
5. For sciatica — most improves with the above over weeks; persistent or severe nerve compression may need further assessment and, occasionally, injections or surgery.
6. When more is needed — persistent pain with a clear structural cause, or significant nerve involvement, may lead to specialist investigation, targeted injections, or surgery in a minority. Surgery is for specific problems (such as significant nerve compression), not for ordinary back pain.
See spine health for keeping the back well between episodes.
At VinayakM in Greater Kailash-1, back pain is assessed by Dr Udit Vinayak (trauma, sports medicine and joint replacement surgeon), with a focus on safe reassurance and active recovery rather than over-investigation:
The goal is a confident return to normal life and fewer recurrences.
Back pain often recurs, but the risk and severity can be reduced:

Stay as active as the pain allows. Prolonged bed rest actually slows recovery and weakens the muscles that support your back. Keeping gently moving, continuing normal activities where possible, and using simple pain relief to help you do so is the modern, evidence-based approach for ordinary mechanical back pain.
Usually not, at least early on. For typical back pain without warning signs, scans often reveal age-related changes that are not the cause of pain and can lead to unnecessary worry and treatment. MRI is reserved for red-flag symptoms, significant or progressive nerve problems, or pain that persists with a suspected specific cause.
Seek urgent care for loss of bladder or bowel control, numbness around the back passage or inner thighs, progressive leg weakness, back pain with fever or feeling very unwell, pain after major injury, or pain with unexplained weight loss or a history of cancer. New severe back pain in an older person with osteoporosis risk also needs assessment.
Most mechanical back pain improves substantially within a few weeks, though it can recur. Staying active, using simple pain relief and, for persistent or recurrent pain, doing a physiotherapy-guided exercise programme give the best chance of a full and lasting recovery. Pain not improving after a few weeks is worth reviewing.
Usually not. Most slipped (herniated) discs and the sciatica they cause improve over weeks with activity, pain relief and physiotherapy. Surgery is considered for a minority — mainly significant or progressive nerve compression, or pain that does not settle despite proper non-surgical treatment — and never as a first step for ordinary back pain.
