
The knee is the largest joint in the body and carries your full body weight with every step, which is why it is one of the most common sites of pain at every age. Pain can arise from several structures: the joint surfaces and cartilage, the ligaments that stabilise the knee, the two menisci (shock-absorbing cartilage pads), the kneecap (patella) and its groove, the tendons above and below the kneecap, or the small fluid-filled sacs (bursae) around the joint.
The pattern of your pain — where it hurts, when it started, what brings it on — usually points to the cause. Pain that builds gradually with age and activity suggests wear-related change; pain after a twist or fall suggests an injury; pain at the front of the knee on stairs and slopes often comes from the kneecap; and pain with marked swelling and heat needs prompt attention.

Knee pain rarely comes alone. Depending on the cause, you may also notice:
Noting these patterns before your consultation genuinely speeds up diagnosis.
Common causes differ by age and situation:
See a doctor promptly if your knee pain comes with any of these red flags:
Without red flags, it is still sensible to be assessed if pain has lasted more than two to three weeks despite rest and simple measures, or if it keeps returning.
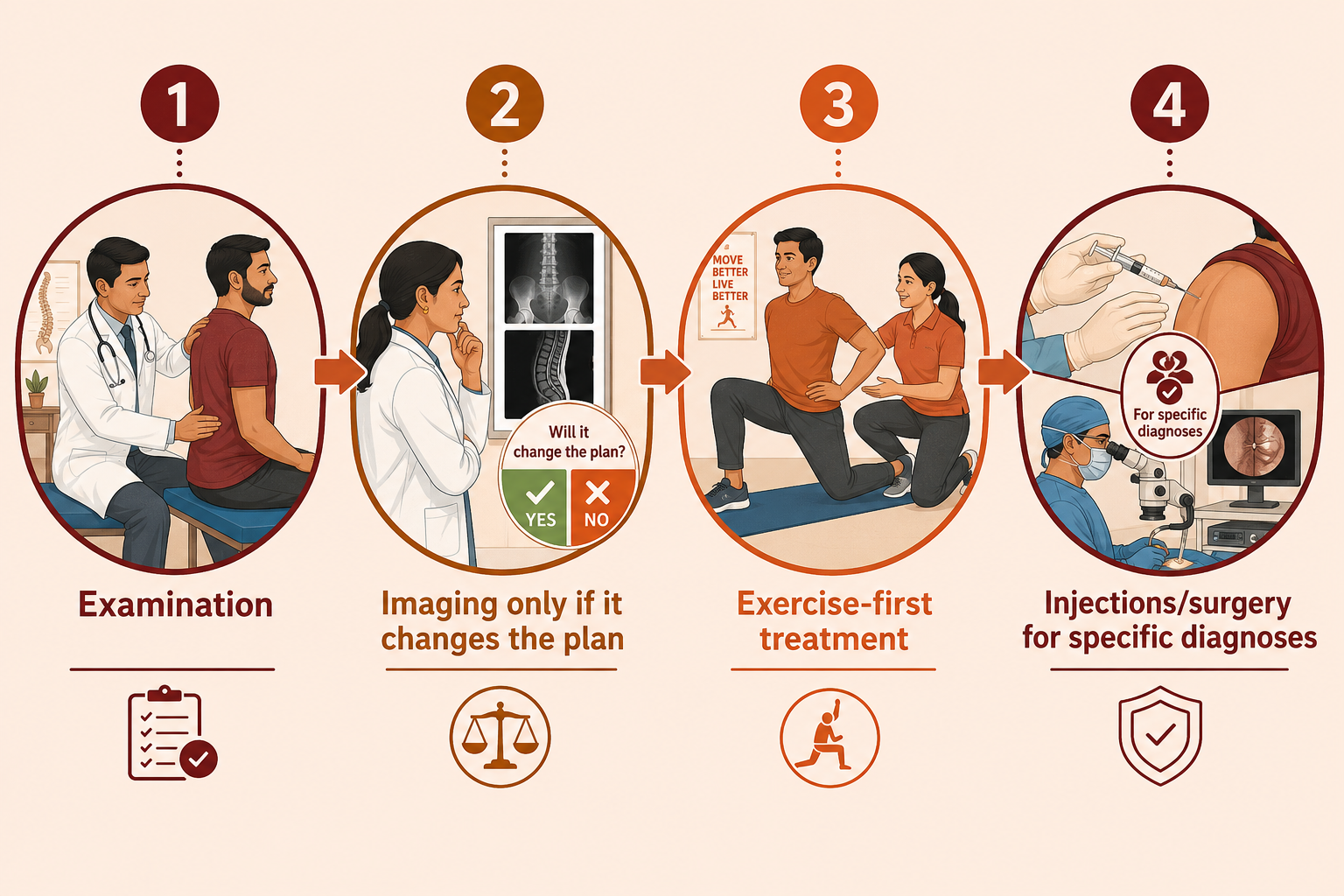
At VinayakM in Greater Kailash-1, assessment of knee pain is clinical first:
The aim is a specific working diagnosis — "knee pain" is a symptom, not an answer.
Treatment depends on the cause, but for most non-emergency knee pain it follows a stepped approach:
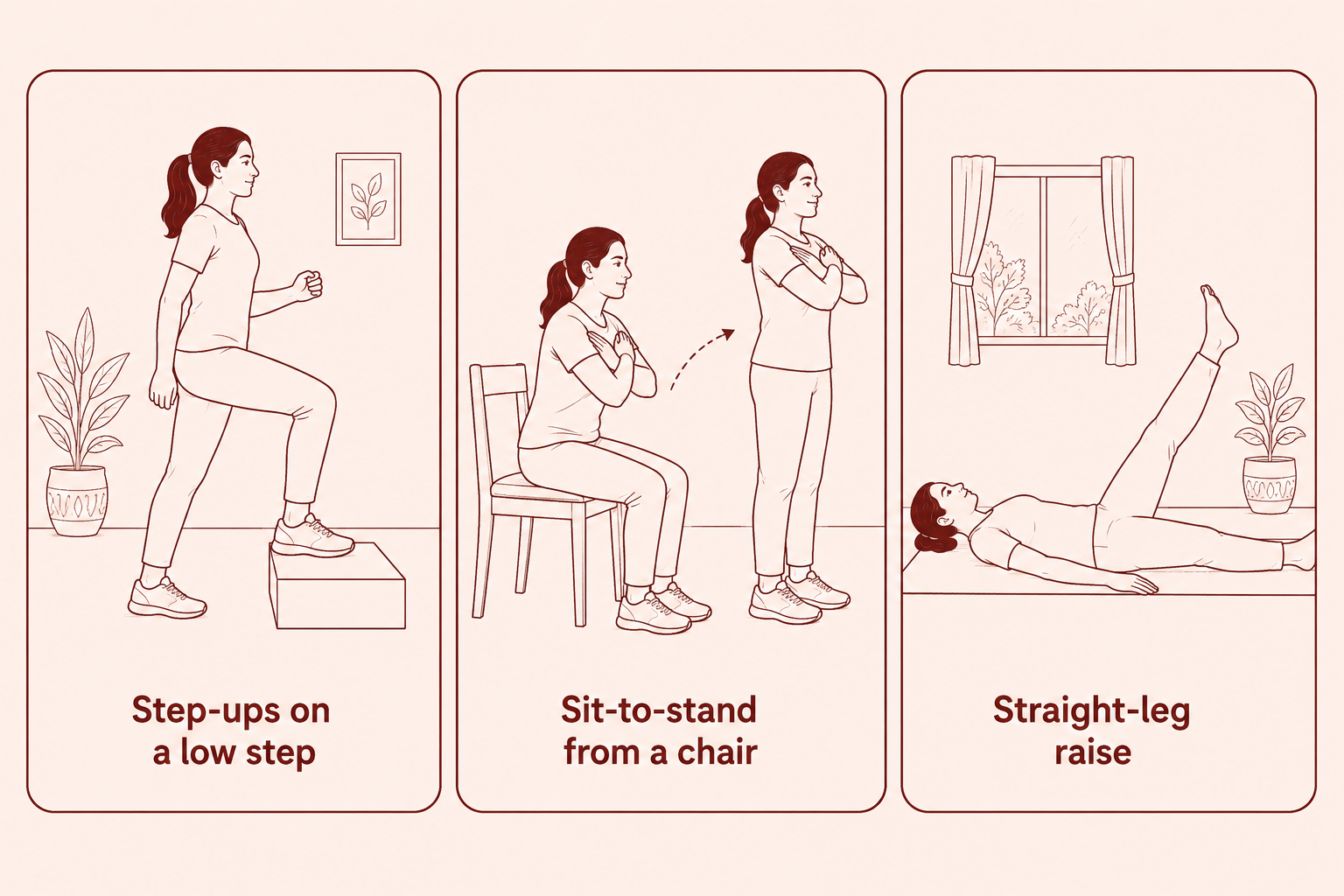
1. First measures (most people, most causes):
2. Cause-specific treatment:
3. Injections and surgery are reserved for specific diagnoses where the evidence and your circumstances support them — they are not shortcuts past the basics.
At VinayakM, knee pain is assessed by Dr Udit Vinayak, a trauma, sports medicine and joint replacement surgeon — which matters, because the full range of options from physiotherapy through keyhole surgery to replacement sits with one clinician, and you are guided to the right step rather than the most invasive one. In practice:
Follow-up is arranged so the plan is adjusted based on how your knee actually responds.
Most knee pain risk is reducible:
Start new exercises gently and stop anything causing sharp or lasting pain; if unsure, ask for a tailored programme.
Seek prompt medical care if the knee is hot, red and swollen (especially with fever), if you cannot bear weight, if the knee is locked or looks deformed, if it swelled rapidly after an injury, or if pain is severe at rest or at night. Otherwise, knee pain that has not improved after two to three weeks of sensible self-care deserves an assessment.
Not always. The examination usually identifies the likely cause. X-rays help when arthritis, alignment problems or fracture are suspected, and MRI is reserved for suspected ligament or meniscus injuries where the result would change treatment. Scanning every painful knee adds cost and worry without improving care.
Pain at the front of the knee on stairs and slopes most often comes from the kneecap and its groove (patellofemoral pain) or from early cartilage wear behind the kneecap. Stairs load this area at several times body weight. Targeted strengthening of the thigh and hip muscles is usually the mainstay of treatment.
Usually yes. For most chronic knee pain, staying active maintains muscle strength and joint nutrition, while complete rest makes the knee weaker and stiffer. The exceptions are acute injuries with red flags, which need assessment first. If a particular distance consistently flares your pain, build up more gradually rather than stopping altogether.
Yes. Hip problems and, less commonly, spine problems can refer pain to the knee — this is well recognised in children and older adults. This is one reason a proper examination covers the hip and back as well as the knee itself.
It depends on the type of tear and your age. Many tears, particularly wear-related tears in older knees, settle with physiotherapy and do not need surgery. Keyhole surgery is considered when the knee locks, when mechanical symptoms persist despite rehabilitation, or for certain tears in younger patients. The decision is individual and should be discussed with a surgeon.
