
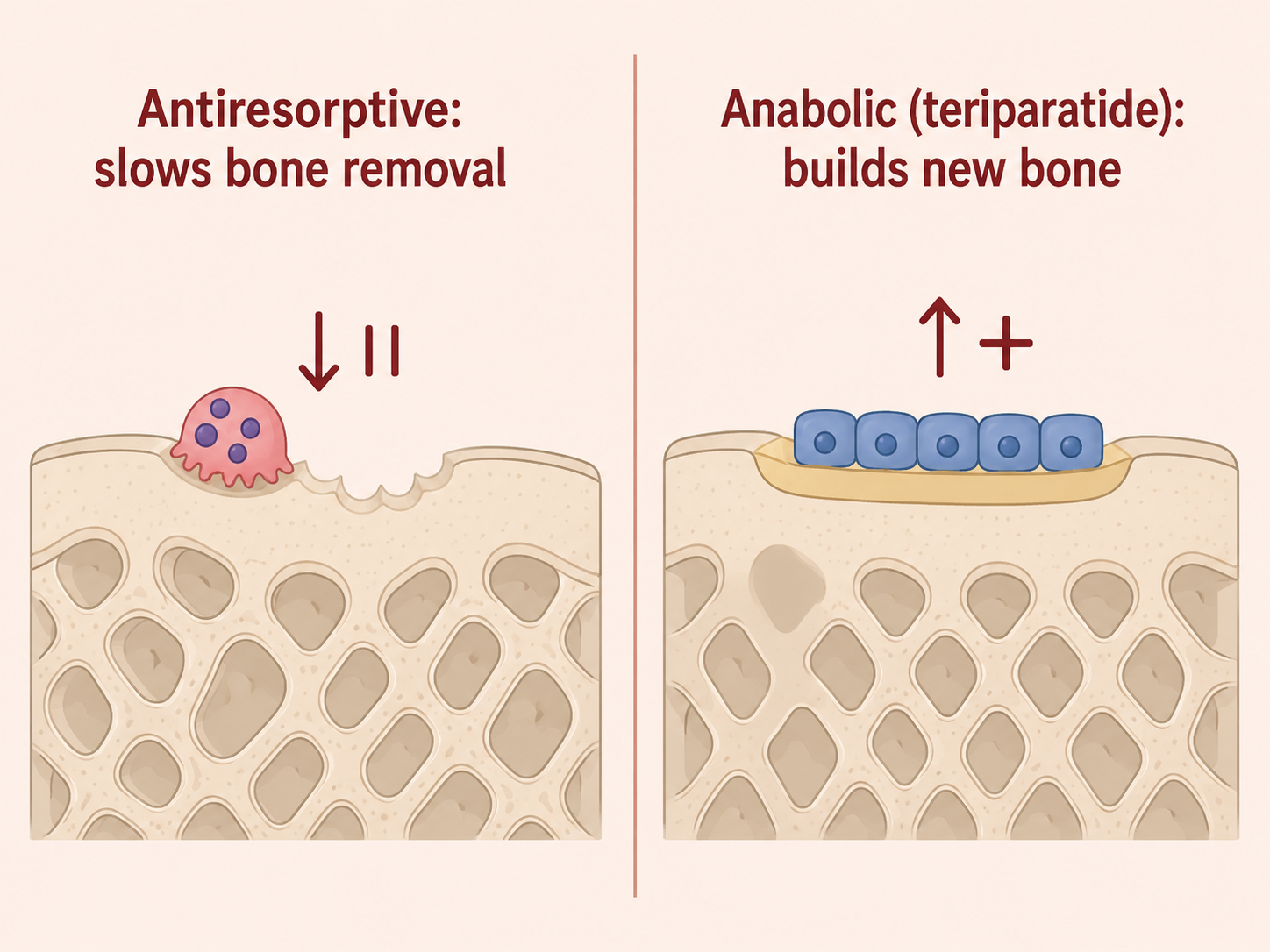
Osteoporosis medicines fall into two broad groups. Most are antiresorptive — they slow the cells that remove bone, so the bone you have is preserved and density gradually improves. A smaller group are anabolic — they actively build new bone. Teriparatide is the best-known anabolic agent.
Teriparatide is a form of parathyroid hormone. Counter-intuitively, given as a once-daily injection it stimulates bone-building cells and increases bone density, particularly in the spine, and reduces fracture risk in severe osteoporosis. Because of its cost, its injection route and the way it is studied, it is generally reserved for more severe disease rather than used first-line, and it is given for a limited course, after which a bone-preserving medicine is usually continued.
This page is an educational overview, not a prescription. Whether any osteoporosis medicine is right for you — and which one — is an individual decision made after assessing your bone density, fracture risk and general health.
This page concerns medicines rather than a condition with symptoms. The relevant question is who osteoporosis medicines, and teriparatide in particular, are for. In general, drug treatment is considered when:
Teriparatide specifically is usually reserved for severe osteoporosis — for example, very low bone density, multiple or spinal fractures, or when other medicines have not worked or cannot be tolerated.
Understanding why these medicines exist comes back to how bone is lost. In osteoporosis, bone removal outpaces bone formation (see bone health and osteoporosis). Medicines address this imbalance in two ways:
The choice between them depends on how severe the osteoporosis is and how quickly bone needs to be rebuilt. For very severe disease, building bone (anabolic) before switching to a preserving medicine is often more effective than a preserving medicine alone — which is the rationale for teriparatide in selected patients.
Discuss osteoporosis medicines with a doctor if you have been diagnosed with osteoporosis, have had a fragility fracture, or have a high fracture risk on assessment. Do not start, stop or source these medicines without medical guidance — dosing, duration and monitoring matter.
Seek prompt care for a suspected new fracture (pain, deformity, inability to use a limb, or sudden severe back pain in an older person). If you are on teriparatide and develop persistent symptoms such as marked dizziness, palpitations or unusual bone pain, contact your doctor.
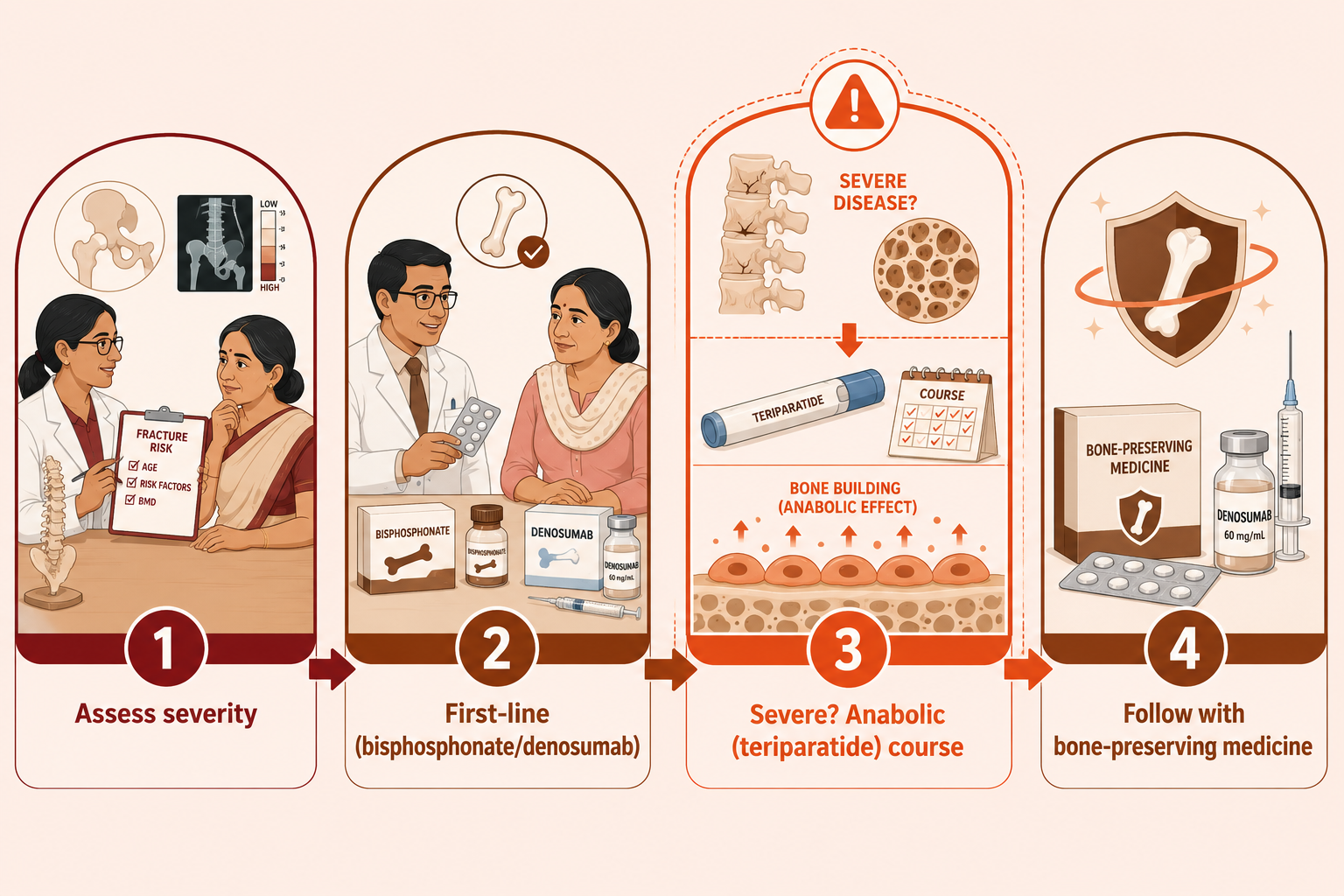
Deciding on osteoporosis medication at VinayakM follows assessment of the underlying condition:
This assessment decides not just whether to treat, but which class of medicine fits your severity and circumstances.
The main osteoporosis medicines, in plain terms:
Using teriparatide:
Alongside any medicine, the foundations still apply: weight-bearing and resistance exercise, adequate calcium and protein, correcting vitamin D deficiency, not smoking, and fall prevention (see bone health). Medicines add to these measures; they do not replace them.
At VinayakM in Greater Kailash-1, osteoporosis medicines including teriparatide are considered by Dr Udit Vinayak (trauma, sports medicine and joint replacement surgeon) as part of a complete fracture-prevention plan, coordinated with your other doctors where needed:
We explain the options in plain language so you understand why a particular medicine is or isn't recommended for you.
The best way to reduce the need for strong osteoporosis medicines is to protect bone before it becomes severely weakened:
Used well, lifestyle measures and timely first-line treatment mean anabolic medicines like teriparatide are needed only by those with the most severe disease.
Most osteoporosis medicines (like bisphosphonates and denosumab) slow the removal of bone, preserving what you have. Teriparatide is different — it actively stimulates new bone formation. Because of this, it is generally reserved for severe osteoporosis or when other treatments have not worked, is given for a limited course, and is usually followed by a bone-preserving medicine.
It is a once-daily injection given under the skin, usually self-administered with a pen device after being shown how. It is prescribed for a limited total duration rather than indefinitely, and calcium and vitamin D are ensured alongside it. Your doctor will explain the schedule and monitoring.
It is not suitable for everyone — certain bone conditions, some cancers or prior radiation to bone, high blood calcium and some other situations make it inappropriate. This is why prescribing is individual and specialist-guided, based on your assessment. Never source or start it without medical supervision.
There is no single best medicine — it depends on your bone density, fracture risk, other health conditions and how severe the osteoporosis is. Bisphosphonates are usually first-line for most people; denosumab and teriparatide have specific roles. The right choice is made individually after assessment, and all work best alongside exercise, nutrition and vitamin D.
Yes, absolutely. Osteoporosis medicines work poorly without adequate calcium, protein and vitamin D, and weight-bearing and resistance exercise remain important for bone and for preventing falls. Medicines add to these foundations rather than replacing them.
